Has health education in the New Zealand curriculum “come of age”?
Jenny Robertson
http://dx.doi.org/10.18296/cm.0005
Abstract
It has been 21 years since a literature review by Helen Shaw established the conceptual foundations for the development of health education as part of the curriculum for New Zealand schools. Using the lens provided by the schooling improvement literature, this article reflects on the development of health education in New Zealand schools to examine two propositions, draw conclusions about the growth and maturity of the subject in relation to curriculum implementation, and report on the challenges still being faced. Recommendations for future developments that have implications for health education teachers, and other education practitioners, policy makers, and researchers working in this field, are discussed.
Introduction
A purposeful search of the curriculum archives on Te Kete Ipurangi (TKI), the Ministry of Education resource website, surfaces a health education literature review written 21 years ago (Shaw, 1994). This review built on the Health Education Syllabus (Department of Education, 1986) and preceded the development of the policy specifications (Ministry of Education, 1995) for the writing of the Health and Physical Education in the New Zealand Curriculum document (Ministry of Education, 1999). The literature review provided direction for the development of the conceptual framework that still underpins the Health and Physical Education (HPE) learning area today. Needless to say, an education document written late last century does not stand up to current education policy and practice in its entirety, with aspects of the review now superseded by newer research and policy, which includes the replacement of the 1999 document with The New Zealand Curriculum (NZC) (Ministry of Education, 2007).
For the purpose of this reflection on health education and curriculum implementation, the “coming of age” title for the article plays on the tradition of many western nations that turning 21 years of age represents an important life milestone, often associated with entry into adulthood and a sign that a certain level of maturity had been reached. It is being used symbolically to convey a sense of the period encompassed by this reflection. The discussion opens with an overview of the schooling improvement literature that provides the conceptual framing for this reflection, followed by a summary of recent New Zealand health education research literature. For the remainder of the reflection the author posits and examines two propositions about the factors that have shaped the growth of health education in New Zealand schools. These propositions have been inconsistently tested and may not stand up with further investigation. However, from the available evidence these claims provide a useful position from which to reflect upon the maturity of health education in NZC. Health education is understood as similar to but distinct from physical education in NZC. Recommendations for future development are made for health-education practitioners, providers, researchers, and policy makers. The intention is to extend the debate about health education in the curriculum.
Schooling improvement
To embark on a reflective exercise that attempts to answer the question “has health education in The New Zealand Curriculum ‘come of age’”? requires a conceptual framework that gives scope for an array of curriculum design and implementation issues to be explored. For this reflection, the field of schooling improvement (or effectiveness) serves this purpose. The substantial body of international and local schooling-improvement literature focuses on research that identifies and describes effective educational leadership and teaching practices—effective in that the practices result in improved and sustained high-quality outcomes for students. These outcomes for students are the academic learning valued by the community, and education-relevant social, cultural, and wellbeing outcomes.
Schooling improvement occupies educational thinking at a global level. The evidence-based policies and practices that constitute schooling improvement are typically (re)articulated for local application. For example, a position paper by Timperley et al. (2009), grounded in international research and theory on school change, sets the scene for schooling improvement in New Zealand. Teacher and leader effectiveness is one aspect of education where a substantial body of research has been synthesised detailing “what works” for teaching and learning. For New Zealand purposes this research is described through the Ministry of Education Best Evidence Synthesis (BES) series (including Robinson, Hohepa, & Lloyd, 2009; Timperley, Wilson, Farrar & Fung, 2007; and Alton Lee, 2003). Teacher effectiveness here refers to capability and capacity of teachers, working in context of their school and community, and with effective leadership, to practice in ways that maximise educational outcomes for their students.
Schooling improvement is inherently political. Abbiss (2013), as editor in this journal, notes that to intellectually understand curriculum change requires embracing “[t]he political nature of curriculum, and the importance of not separating curriculum from the structures and wider political changes within which it is embedded” (Abbiss, 2013, p2). Curriculum for the purpose of this reflection is a matter of policy and consequently it comes with intended meanings, although those meanings are only given direction in NZC and are not stringently prescribed.
The reason for this choice of framework is that to talk of health education “coming of age” implies that the curriculum has been enacted and implemented. The context in which this happens for most educational leaders, teachers, and students in New Zealand is through state funded education. State funded schools are required to be responsive to the New Zealand Education Act 1989, as directed through current policies and strategic approaches that seek to improve outcomes for all students. A key measure of schooling improvement is student achievement in and across the curriculum, regardless of the context (or subject) for learning, and health education is integral to this.
By adopting a schooling-improvement conceptual lens the assertion is being made that subject maturity is a function of how well a learning area (in this case the subject of health education in the Health and Physical Education learning area), in context of wider curriculum and schooling considerations, has been implemented. This framework has also been selected in preference to one that is specific to health education knowledge or pedagogy for pragmatic reasons. As will be discussed, the body of New Zealand-specific literature needed to frame an exclusively health education debate is, at present, very small, making it difficult to sustain an argument embedded only in this aspect of NZC. Until the local situation is better understood, making meaningful links with international understandings of health-education knowledge, pedagogy, and student outcomes remains problematic.
Timperley et al. (2009) note that “pieces of paper are poor mechanisms for change” (p. 4). NZC and the resources that support it represent some of these pieces of paper. Until people implement curriculum (whereby teachers teach and students learn, and teachers learn and students “teach”), subject maturity cannot happen. Hence it is the position of this reflection that the debate about maturity must extend beyond the pieces of paper on which (the) curriculum and health education ideas are written, and to give focus to the practices of teachers and outcomes for students.
New Zealand health education research and theoretical literature
It is acknowledged that New Zealand-specific literature on health education, as a subject in NZC, has seen growth in very recent years. However, the relative paucity of local theoretical and research-based literature means that describing the current state of health education, and presenting a debate about New Zealand health education developments for academic purposes, is still a considerable challenge. Little of this literature speaks purposefully or deliberately to a schooling-improvement agenda, although aspects of some reporting can be interpreted through this lens. Overall, this relatively small body of research literature could be seen as an indicator of a subject still in development.
Post-NZC contributions to the local literature include: context specific research such as sexuality education (Allen, 2011); the use of the philosophy of hauora (as a concept of wellbeing) in English- and Mäori-medium curricula (Heaton, 2011); consideration of cultural perspectives in health education (Fitzpatrick, 2009); consideration of the role of external providers in HPE programmes (Petrie, Penney & Fellows, 2014); illustrating aspects of critical pedagogy in practice (Fitzpatrick & Russell, 2013); teachers perceived value of health education (Hargreaves, 2012); teaching health education at tertiary level (Cushman, Brown Hajdukova, & Clelland, 2015); reframing health education for schooling purposes (Quennerstedt, Burrows, & Maivorsdotter, 2010, Sinkinson & Burrows, 2011); and theorising about health education as a discipline of study (Fitzpatrick 2014). Highlighting the ongoing confusion of the purpose of health education as it is positioned in NZC occupies the writing of Burrows & McCormack (2012), Powell & Fitzpatrick, (2013), Burrows & Sinkinson, (2014), and Fitzpatrick, & Tinning, (2014).
Periodically the Ministry of Education produces guiding documents to show schools how to bring together various policy level requirements with evidence-based best practice. The revised Sexuality Education: Guide for Principals, Boards of Trustees and Teachers (Ministry of Education, 2015) and the Alcohol and Other Drug Education Programmes Guide for Schools (Ministry of Education, 2014a) are recent examples of such guidelines. Secondary student achievement in health education for the National Certificate of Educational Achievement (NCEA) is reported annually by the New Zealand Qualifications Authority (NZQA) (NZQA, n.d.b), and for primary schools by the National Monitoring Study of Student Achievement (NMSSA, 2014). The Education Review Office (ERO) is the government body responsible for reviewing and reporting schooling effectiveness in New Zealand. The last ERO report specific to health education was around sexuality education (ERO, 2007). In conjunction with the trialling of a set of draft wellbeing indicators (ERO, 2013), national reporting in 2015 gave focus to student wellbeing in primary and secondary schools which included consideration of the place of health education in the promotion of wellbeing at school (ERO, 2015a, 2015b). Such reports and guidelines have particular foci, reflecting governmental and political interests.
Evidence for the reflection
With limited local health education specific research literature that explicitly supports a schooling improvement debate, the sources of information providing context and evidence for this reflection, and the basis for the following propositions, come predominantly from education practitioner sources such as: the HPE community on TKI and the NZC archive of this online resource; Education Counts (the Ministry of Education research website); NZQA; ERO; the New Zealand Council for Educational Research (NZCER); the New Zealand Health Education Association (NZHEA); and health education teaching and learning resources developed by the Ministry of Education, non-government organisations (NGOs), and resources produced by teachers which are commercially published or informally produced and shared around teacher networks. Specific examples of these resources are included with the following discussion.
Propositions
Proposition one: The underlying concepts define health education knowledge
Explicitly incorporating the underlying concepts of the HPE learning area of NZC in teaching and learning resources, and developing teachers understanding of these concepts, has been the most important development shaping and advancing what constitutes health education knowledge, skills, and understanding.
Underlying concepts of HPE
The Shaw (1994) literature review provided the foundation for what became the underlying concepts of the Health and Physical Education in the New Zealand Curriculum (Ministry of Education, 1999) document. Although not framed as “underlying concepts” as such at the time, Shaw highlighted the need for a curriculum that considered a socio-ecological approach, health-related attitudes and values, Mäori and other cultural values towards health, and health promotion. Each of these ideas was translated into the policy specifications for development of the HPE curriculum statement. The (then) Christchurch College of Education writing team that won the contract to develop the draft document used these ideas to provide the conceptual framework for the learning area (Tasker, 1996/7). With no recommendations for change to this conceptual foundation being made in the curriculum stocktake report (Le Métais, 2002), these concepts remained when the Health and Physical Education learning area statement was developed for NZC, published in 2007.
Through resourcing that unpacks the intent and “essence” of the learning area (NZC pp. 22–23), teachers and students of health education have been introduced to the idea that the underlying concepts are the “big ideas” that frame all health-education knowledge. Application of these concepts grows increasingly complex across the levels of the learning area (NZC Levels 1–5 typically cover the first 10 years of schooling, and NZC Levels 6–8 map onto NCEA Levels 1–3, upon which Year 11–13 programmes are based). At lower levels of the curriculum students are “participating’, “identifying” and “describing”, and as their learning develops across the levels they learn to “critically analyse” health-related situations.
A range of resources exist to support teachers teaching health education. For example, resources developed by NGOs such as Family Planning (the various titles in the Hei Huarahi and Sexuality Road series covering Years 5–10 (Family Planning n.d.)), and Mental Health Foundation (Mental Health Matters (Robertson, 2009); Change, Loss and Grief (Dickinson & Tonkin, 2000)); the Ministry of Education developed resources such as the Curriculum in Action series (TKI, n.d) developed for primary and secondary schools to support the 1999 HPE document (currently under review and redevelopment); teaching resources such as Caring for Yourself and Others (Tasker 1998); Social and Ethical Issues in Sexuality Education (Tasker 2000); Social Issues: Alcohol (Tasker and Hipkins, 2002); and commercially produced learning workbooks and NCEA study guides for students (Dixon and Robertson, 2011; Dixon and Robertson, 2012; Hedges and Robertson, 2014; Robertson and Dixon, 2014) supplement officially produced NZQA assessment materials. In various ways these resources show teachers how the underlying concepts are incorporated into health education teaching and learning programmes and develop across the levels. In addition, matrices of learning intentions developed with the sexuality education (Ministry of Education, 2015) and drug education (Ministry of Education, 2014a) guides indicate how the concepts are applied in these contexts.
The ways these HPE underlying concepts are intended to be used and developed in secondary schools are briefly described.
Hauora and wellbeing: A holistic understanding of health has been promoted by the World Health Organization (WHO) since 1948. WHO describe health as “a state of physical, mental and social wellbeing and not merely the absence of disease or infirmity” (WHO, 1948). To give focus to the health needs of Mäori, the conceptualisation of health presented by Durie (1998) through the philosophy of hauora, was adopted for the New Zealand curriculum. It is noted that the inclusion of a Mäori philosophy of wellbeing in an English medium document is not fully supported. Heaton (2011) in this journal highlights some of these issues. Earlier reporting by Salter (2000) and Hokowhitu (2004) challenged the way the concept of hauora was used in context of the HPE learning area and questioned how the colonial adoption and use of this concept variously reframed or sanitised its use. However, as this critique was physical-education specific and preceded NZC these ideas warrant revisiting and with specific relevance to health education, and in learning contexts like mental health and sexuality education that dominate the subject. Also needing consideration is the way the other underlying concepts have defined and shaped the use of hauora as a concept of wellbeing. Concerns and critique aside, the concept of hauora, as interpreted through Durie’s te whare tapa whä (the four-sided house) model (Durie, 1998; Ministry of Education, 1999) has become widespread across the health and social sectors over the past decade, as evidenced by the way the Ministry of Health for example promotes the use of the term and concept for application across many health developments (Ministry of Health, 2015).
The previously listed teaching resources would suggest that in most secondary school learning programmes, hauora and wellbeing likely represents the first of the underlying concepts that students deliberately learn about in health education. At secondary school, students unpack the physical, mental and emotional, social, and spiritual dimensions of wellbeing in relation to different contexts, to develop breadth of understanding of the ways health and wellbeing can be described. Importantly they learn how the dimensions interrelate and the need to maintain balance between the dimensions, giving focus to a “holistic” understanding of wellbeing. There was an unfortunate tendency in early NCEA developments to conflate the meanings of hauora and wellbeing, and to personalise the use of the term to talk about “my hauora”, and that hauora is “changed” or “affected” by a range of issues, rather than using the term hauora as a concept (which doesn’t change) through which wellbeing is described. This oversight is still being remedied with a number of HPE learning area and NCEA resources (for example) still using the term hauora synonymously with wellbeing and in a personalised way. The hypothesis needs testing but it would appear likely that most students are now leaving secondary school with a holistic understanding of wellbeing and understanding of the whare tapa whä model of hauora. This represents an outcome for students.
Socio-ecological perspective (SEP): The terminology of the SEP was established with Shaw’s (1994) review based primarily on the writing of Lawson (1992). Unpacking the complexities of the SEP became essential for “levelling” NCEA and stepping up the conceptual development of health education knowledge upon which NCEA achievement judgements could be made. To this end students were introduced to the notion that the SEP comprised interrelated considerations of the personal (individual, self), interpersonal (communication and interactions between people), and community or societal factors (population level). To refine this understanding at NCEA Levels 2 and 3, an evidence base was added to this knowledge whereby students are introduced to the WHO determinants of health (see Tasker & Hipkins, 2002; Making Meaning Making a Difference (MMMD), Ministry of Education, 2004). Students working at lower levels of the curriculum are gradually introduced to the language of these conceptual ideas, as relevant to the learning contexts selected for their health-education programme.
Health promotion: As a concept, health promotion is part of the knowledge of health education, focusing on how to take action individually and collectively to support the wellbeing of self, others, and communities. Teachers and students are encouraged to use the action competence cycle (Tasker, 2000; see also Ministry of Education, 2004, p. 28) a type of inquiry-learning process, to frame health promotion planning and actions. A paper prepared by Robertson (2005) explained health promotion as a health-education concept. In preparation for Level 3 NCEA health education, MMMD (Ministry of Education, 2004) offered teachers and students an entry-level understanding to internationally understood health-promotion models which, for convenience, have come to be known as the “health education models”. The Ottawa Charter (WHO, 1986), referenced in the 1999 HPE document, provided a focus for seeing health promotion as a publicly shared health responsibility. The subsequent Bangkok Charter (WHO, 2005) which makes health a global responsibility, and Durie’s Te Pae Mahutonga (the Southern Cross) model (Durie, 2003), have not yet informed health education knowledge development as much as they could. These models offer potential for further conceptualisation of health promotion for learning in health education, and for whole school (and community) approaches to wellbeing.
However, the conflation and confusion of health promotion as a practice (with its own set of outcomes), as distinct from the models of health promotion for health education used in conceptual teaching and learning, highlights a major tension around the purpose of health education when it sits in a curriculum. The Ministry of Education review of alcohol and other drug education programmes (Robertson, 2013) highlights some examples of these health education/health promotion tensions. Research by Fitzpatrick, & Tinning (2014), Powell & Fitzpatrick (2013), and Burrows & Sinkinson (2014), variously reports what happens when curriculum intentions and educational learning outcomes, and health promotion (health behavioural outcomes) are not clearly understood by teachers, or those working in the health and social sectors. For schooling-improvement purposes, these studies are helpful for identifying where misunderstandings lie and what is getting in the way of improving educational (learning) outcomes for students.
Health education teachers assess student learning and application of health promotion understandings and processes, and participation in health-promoting processes and actions. They do not judge student achievement or their own teacher effectiveness on successful health promotion (health status or behavioural) outcomes. However, a whole-school approach to promoting schooling relevant aspects of wellbeing (where there is a collective responsibility of all members of the school community to reduce bullying or be inclusive of diversity for example) may seek to achieve health or wellbeing (behavioural) outcomes.
Attitudes and values (A&V): “Attitudes and values” is not so much a concept of itself, but when selected A&V are applied to situations, they can be used as a “big idea” that help to decide which health-promoting actions show care, consideration, and respect for self, others, society and the environment, or which actions reflect the values of social justice. The A&V of the learning area have given direction to what is, and is not, acceptable health-education knowledge. For want of a better explanation A&V help decide which knowledge is acceptable or unacceptable. This means, for example, that any teaching and learning that shows a lack of inclusiveness of diversity does not belong in the curriculum. This position is further supported by the values statement in NZC that overarches all teaching and learning in the curriculum.
Social justice remains one of the more underdeveloped aspects of the A&V and teaching resources. The NCEA achievement standards and supporting resources would indicate that it is usually NZC Level 7 (about Year 12) before students are explicitly introduced to the idea. Social justice is itself a complex concept so the learning focus is given guidance by being limited to what’s fair, inclusive, and non-discriminatory, ideas that are gradually developed across the levels of NZC.
The underlying concepts in combination: There is (arguably) no prescribed content knowledge in health education—it is a learning area framed by big ideas applied to selected contexts. If anything, the underlying concepts become some of the “content” knowledge students learn in secondary school courses. As health education as a subject has developed, the resourcing shows how these underlying concepts have become mutually defining. Students learn how the various dimensions of wellbeing are interrelated, and how the personal, interpersonal and societal aspects in combination reflect the SEP concept. They also learn how the underlying concepts intersect and give shape to the meaning of the other concepts, such as how some health-promoting actions are more acceptable because of the way they reflect the values of social justice, and require individual and collective responsibility.
As health education has developed as a knowledge area and a curriculum subject, it has also been necessary to introduce another layer of health education-specific concepts related to the main contexts for learning. These include concepts related to sexuality and gender, resilience, and harm minimisation (as applicable to alcohol and other drugs). This development has been important to add depth of knowledge to learning so that expected high-quality student learning outcomes can be achieved.
Contexts for learning in health education: The contexts for learning in health education are framed by the seven Key Areas of Learning (KALs), three of which dominate secondary school health education—mental health, sexuality education, and food and nutrition. These contexts alone do not constitute health education in NZC. Without the conceptual treatment discussed above, they are simply collections of content knowledge about a health topic. The HPE (Ministry of Education, 1999) document dedicated pages of text explaining the scope of each of these KALs. The loss of these statements from NZC (Ministry of Education, 2007) has caused some concern but the older document remains a valid source of information describing the intent of the KALs.
The question of maturity: High-quality student outcomes require teachers to have comprehensive understanding of the conceptual knowledge of their specialist learning area in the curriculum. Therefore any judgement of maturity cannot help but consider how well these underlying concepts are understood and incorporated into teaching and learning programmes, and the assessment of student learning resulting from these programmes. Comments in annually published NZQA health education examiners and moderators reports (NZQA, n.d.a) repeatedly note how poorly developed the underlying concepts are in assessment material submitted by many students. This problem has persisted since NCEA was introduced in 2002.
Observations on the maturity of health education in terms of its conceptual and contextual knowledge foundations depend on the perspective taken. On the one hand, and from a policy perspective, the curriculum is seen to have teaching and learning resources that show in various ways how the conceptual and contextual intent of learning area is fulfilled, and there is an NCEA achievement standard matrix that makes explicit use of the underlying concepts developed through to the highest level of the curriculum. On the other hand, and from a methodological perspective, it might be observed that there is no known research theorising or critiquing the way the combination of the underlying concepts have shaped health education knowledge in NZC which has taken shape largely as a grassroots development by the educational practitioners teaching students in schools.
Proposition two: NCEA has established health education as a pathway to meaningful qualifications
The development of NCEA, New Zealand’s national school qualification system generally for students in Years 11–13, has been highly influential in shaping health education as a learning pathway.
Health-education-specific achievement data is available for secondary-school students through NCEA results, and for primary-school students through the University of Otago, National Monitoring Study of Student Achievement (NMSSA) (previously the National Education Monitoring Project, NEMP, see Flockton & Crooks, 2006). A key finding of the 2013 NMSSA report (NMSSA, 2014), the first for HPE since the release of NZC, was that over 95 percent of Year 4 students were achieving in HPE at Level 2 of NZC in HPE (the expected achievement level of a student making adequate progress through the curriculum), but by Year 8 only 50 percent of students were achieving at the expected NZC Level 4. From a schooling improvement perspective, this is a major concern as it means many students are arriving at secondary school (Year 9) without the depth of HPE understanding that would signal that they are on track for NCEA success at secondary level.
The NCEA system is explained fully on the NZQA website (NZQA n.d.b). NCEA Level 1 was introduced in 2002, and Levels 2 and 3 were phased in over the following 2 years. NCEA was highly influential for advancing the development and understanding of health education in NZC. The development of senior secondary specific resources such as those developed by Tasker (2000) and Tasker & Hipkins (2002), along with NZQA and the Ministry of Education developed resources to accompany the achievement standards, in a sense forced the development of health education at senior secondary level. Health education has had a three-level, 24 credits per level, matrix of achievement standards covering Levels 6-8 of NZC since the beginning of NCEA (NZQA n.d.a). The way the achievement standard matrix develops across Levels 1–3 is documented in the senior secondary guides (Ministry of Education, 2013). However, it requires detailed analysis of a range of teaching, learning, and assessment resources to work out how NZC and NCEA levels step up conceptually.
NCEA proved to be a double-edged sword. In its favour it gave health education status as a subject in the senior school curriculum, and it provided students with another option for a learning pathway beyond Year 10. However, with no established history in senior secondary schooling, it meant the achievement standards quickly became the default curriculum and teachers tended to plan learning programmes primarily to the standards, and less so the overall intent of NZC. This was apparent in the resources prepared for the (now defunct) Ministry of Education Beacon Schools Project that supported the early development of senior secondary health education, a project described by Tasker (2006), and prevails through NCEA support materials such as the study guides and learning workbooks cited previously. This situation is not unique to health education with Hipkins (2013) reporting that the problem of NCEA driving the curriculum was still a major issue in secondary schools generally.
The question of maturity: It could be said that the very fact New Zealand has national qualifications in health education, through to the highest levels of the curriculum, is a measure of subject maturity. Student achievement outcomes in health education are measured in the same way as all other subjects. However, maturity would appear to be some way off when considering the status and recognition of the subject for its academic learning, and the proportions of students opting to take health education courses at senior level and achieving well in these courses, as evidenced by the following situations and data.
Scholarship: The scholarship assessment is the highest level of academic achievement New Zealand students can attain at secondary school (NZQA, 2014). It rewards students who can demonstrate deep knowledge and critical insight, and can be gained in most NZC subjects. In 2014, and for the third consecutive review cycle, health education was denied a health education-specific Scholarship assessment similar to most other subjects that derive from Level 8 of NZC. Instead, it has been made possible for health education students to complete a report that meets the requirements of the redeveloped physical education Scholarship. If such a report is judged to be among the top few percent, the (health education) student can be awarded physical education Scholarship. The physical education Scholarship standard limits health education students’ selection of topic. The implications of this decision are still being investigated.
Recognition at tertiary level: The establishment of health education as a subject with a meaningful learning pathway leading to degree-level tertiary courses, is yet to be widely understood and supported. The Vocational Pathways Profile Builder (Ministry of Education, 2014b) illustrates the value of the subject and includes health education standards in many study and career pathways. However, the absence of the subject on most New Zealand university preferred-subject lists, recommended or required for entry into courses, means health education still struggles for recognition by universities as a subject leading to courses spanning the social sciences, health, and education.
NCEA entry and results: Another possibility for judging subject maturity, relevant to the schooling improvement framework, is to consider rates of NCEA entry and achievement results. NCEA data from 2013 and 2014 are provided in Table 1 below (NZQA 2013, 2014). Most students do not complete all standards at each level. The standards most commonly excluded from a programme are the externally assessed standards. There is a trend in secondary schools to avoid over-assessing and by offering 18–20 credits in a year-long course, meaning the combination of standards that a student completes is unique to them are varied and makes population level analysis a complex task. Analysis of these data are further confounded when Year 11, Level 1 programmes often combine a selection of health education and physical education standards in one course, and the fact that NZQA have successively changed the way achievement statistics are publicly reported since NCEA began.
Table 1. Comparison of 2013 and 2014 NCEA health education results
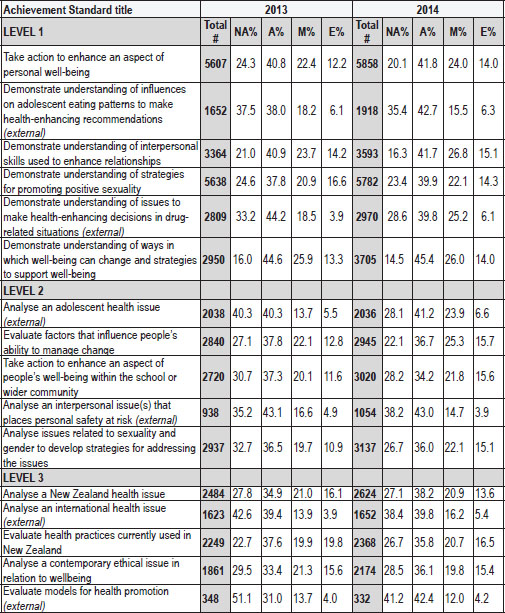
Source: NZQA Statistics (NZQA, 2013, 2014)
Total # = total number students completing the assessment for the standard in the current year.
NA = Not achieved, A = Achieved, M = Achieved with Merit, E = Achieved with Excellence.
External = External assessment (examination), all other standards are internally assessed.
Trends in the 2013–2014 data indicate that: there has been a modest increase in the numbers of students completing most health education standards indicating a growing popularity of the subject overall; however the numbers of students taking health education (assessed by achievement standards) drops off between Levels 1 and 2 which may be suggesting students’ perceived value or usefulness of the subject for qualifications pathways reduces, or that they don’t have access to senior health education courses; internal assessments are far more popular than external assessments (at least one external assessment is required for course endorsement, a recognition of overall high performance); the most popular Level 1 standards are the internally assessed personal goal-setting and sexuality standards with over 5000 students completing these assessments in 2013 and 2014 (noting that the cohort participating in Level 1 NCEA in each of these years was over 40,000 students), and about 70–80 percent of students achieving each standard; and rates of Not Achieved are higher, and Excellence lower, in the external assessments compared with the internal standards, a trend that challenges, for example, the perceived status of the subject as an academic pathway to higher education that places value on examinations.
What constitutes maturity in terms of NCEA enrolment and achievement rates is open to interpretation and requires comparison with other subjects and further investigation. It would be reasonable to suggest that these results are indicating a need to improve the capacity of teachers to teach effectively to the highest levels of the curriculum, and to enhance the profile of health education in schools as a viable pathway to meaning qualifications that lead to further study and careers.
Conclusion and recommendations
For professional teachers and educational leaders seeking to maximise educational outcomes for students, in accordance with the goals and principles of schooling improvement, curriculum does matter. Understanding (the) curriculum is central to educational practice and judgements of teacher and schooling effectiveness. However, the fact that NZC sets the direction for teaching and learning, and that it is not a prescribed body of knowledge to be transmitted, means HPE in NZC is open to interpretation. At times this interpretation is at odds with the intent of the curriculum (both the HPE learning area and NZC in its entirety), and the policy-driven requirements of schooling.
Many aspects of health education in NZC remain under-theorised and under-investigated in the academic literature. Without access to a substantial and detailed body of locally relevant, health education-specific research evidence, it becomes a challenge to sustain an argument seeking to make a clear case for (or against) the maturity of health education in NZC. Rather than attempt to present a defensible and definitive answer to the question that titles this article, a list of recommended actions is instead provided for the future growth and development of health education, based on the discussion presented in this reflection.
In the evidence-driven practice of teaching and educational leadership, and the high level demands for schooling improvement, there is a need to theorise and conceptualise health education in its NZC context. Researchers are presented the challenge to respond to and further test the claims made in this article, and to revise and update earlier (pre-NZC) health education thinking and understanding. When investigating context-specific aspects of health education, it is essential that researchers understand the policy-driven intent of the curriculum and the schooling context in which this learning sits. A deepened understanding about the underlying concepts that frame health education knowledge, and possible alternative interpretations, will also be vital for informing curriculum review in the future.
Although not extensively discussed in this reflection, but identified as a recurrent (and perhaps unintended) feature of the local research literature, there is a need to develop critical insight and clarity around the assertion that health education in NZC is “about” health. The measurable outcome of health education in NZC is about learning knowledge, skills and understanding related to health—knowledge which may make a contribution to community or national health promotion goals (but in isolation will not achieve desired population-level health outcomes). Whereas education “for” health (that is, health promotion) where the outcome is focused on wellbeing and health behavioural outcomes is the collective responsibility of schools and whole communities.
There are many actions that teachers, and senior and middle leaders (Ministry of Education, 2012), and professional learning and development (PLD) providers can engage in to support the development and maturation of health education, as a valuable learning pathway for students. These actions include the following.
•Ensuring teachers have high-quality conceptual and contextual knowledge of the subject so that students have access to the type of learning that provides them with the range of knowledge and skills that will allow them to achieve their learning goals.
•Designing teaching and learning programmes and selecting resources that reflect the diverse identities and backgrounds of students and which respond to learning pathways needs.
•Supporting senior leaders to see the potential for health education as an integral and valued part of the school curriculum and advocate health education pathways to meaningful school-level qualifications, tertiary study and careers.
External agencies that provide resources and support for in-school delivery of health education material need to partner with education institutions to ensure that they understand NZC and the teaching and learning environment in which they expect their resources or programmes to be used.
Returning to the question that gave this article its title, “has health education in The New Zealand Curriculum come of age?”, the limited evidence so far would suggest not (yet). At present, being part of health education feels like being trapped in an awkward state of mid-adolescence—poorly understood, struggling to establish an identity, often in trouble, and uncertain of the future. In closing it is perhaps more constructive to make use of the popular saying that “30 is the new 21”. It suggests health education has met a certain level of maturity insofar as the subject is seen for its potential and promise, but that there is still some growing up to do. It will take some years yet to reach a level of maturity whereby health education can assert its independence, have its own unique identity, be autonomous of other subjects (but at the same time complimentary to other bodies of knowledge and understanding), make its own decisions, and sustain itself.
References
Abbiss, J. (2013). Making sense of curriculum. Curriculum Matters 9, 1–7.
Allen L. (2011). Young people and sexuality education: Rethinking key debates. Basingstoke, England: Palgrave Macmillan. http://dx.doi.org/10.1057/9780230297630
Alton Lee, A. (2003) Quality teaching for diverse students in schooling: Best evidence synthesis iteration (BES). Wellington: Ministry of Education.
Burrows, L., & McCormack, J. (2012). Teachers talk about health, self and the student “body”. Discourse: Studies in the Cultural Politics of Education, 33(5), 729–744. http://dx.doi.org/10.1080/01596306.2012.696502
Burrows, L., & Sinkinson, M. (2014). Mental health in corporeal times. In K. Fitzpatrick & R. Tinning (Eds.), Health education: Critical perspectives (pp. 156–170). Oxford, England: Routledge.
Cushman, P., Brown Hajdukova, E., & Clelland, T. (2015). Moving towards a holistic paradigm: Teaching sexuality education in a New Zealand university. British Journal of Education, Society and Behavioural Science, 9(4), 265–276. http://dx.doi.org/10.9734/BJESBS/2015/17891
Department of Education. (1986). Health education syllabus. Wellington: Department of Education.
Dixon, R. and Robertson, J. (2011). Level 1 health education learning workbook. Auckland: ESA.
Dixon, R. and Robertson, J. (2012). Level 2 health education learning workbook. Auckland: ESA.
Durie, M. (1998). Whaiora: Mäori health development (2nd ed.). Auckland: Oxford University Press.
Durie, M. (2003). Ngäkahui pou: Launching Mäori futures. Wellington: Huia Publishers.
Education Council of Aotearoa New Zealand. (2009). Practicing teacher standards. Wellington: EDUCANZ.
Education Counts. (2015). Education counts [website]. Retrieved from http://www.educationcounts.govt.nz/home
Education Review Office (2007). The teaching of sexuality education in years 7–13. Wellington: ERO.
Education Review Office (2013). Wellbeing for success: Draft evaluation indicators for student wellbeing. Wellington: ERO.
Education Review Office (2015a). Wellbeing for children’s success at primary school. Wellington: ERO.
Education Review Office (2015b). Wellbeing for young people’s success at secondary school. Wellington: ERO.
Family Planning (n.d.). Teaching resources. Retrieved from http://shop.familyplanning.org.nz/teaching-resources
Fitzpatrick, K., & Russell, D. (2013). On being critical in health and physical education. Physical Education and Sport Pedagogy, 20(2), 159–173. http://dx.doi.org/10.1080/17408989.2013.837436
Fitzpatrick, K., & Tinning, R. (2014). Health education’s fascist tendencies: A cautionary exposition. Critical Public Health, 24(2), 132–142. http://dx.doi.org/10.1080/09581596.2013.836590
Fitzpatrick, K. (2009). Indigenous perspectives in HPE curriculum: Contradictions and colonisation. In M. Dinan-Thompson (Ed.), Health and physical education: Issues for curriculum in Australia and New Zealand (pp. 120–143). Melbourne, VIC: Oxford University Press.
Fitzpatrick, K. (2014). Critical approaches to health education. In R. Tinning and K. Fitzpatrick (Eds) Health education: Critical perspectives. Oxford, England: Routledge.
Flockton, L. & Crooks, T. (2006) Health and physical education assessment results 2006. Report #40. Wellington: Ministry of Education Educational Assessment Research Unit.
Hargreaves A. (2013). The perceived value of health education in schools: New Zealand secondary teachers’ perceptions. Journal of Curriculum Studies, 45(4), 1–23. http://dx.doi.org/10.1080/00220272.2012.675356
Heaton, S. (2011). The co-opting of hauora into curricula. Curriculum Matters 7, 99–117.
Hedges, K., & Robertson, J. (2013). Year 9 & 10 health education learning workbook. Auckland: ESA.
Hipkins, R. (2013). NCEA one decade on: Views and experiences from the 2012 NZCER National Survey of Secondary Schools. Wellington: New Zealand Council for Educational Research.
Hokowhitu, B. (2004). Challenges to state physical education: Tikanga Mäori, physical education curricula, historical deconstruction, inclusivism and decolonisation. Waikato Journal of Education, 10, 71–84.
Lawson, H.A. (1992). Towards a socio-ecological conception of health. Quest, 44, 105–121. http://dx.doi.org/10.1080/00336297.1992.10484044
Le Métais, J. (2002). New Zealand stocktake: An international critique. Slough, England: National Foundation for Educational Research.
Ministry of Education. (1995). Policy specifications for a national curriculum statement in health and physical education. Retrieved from http://health.tki.org.nz/Key-collections/Curriculum-development/Policy-specification
Ministry of Education. (1999). Health and physical education in the New Zealand curriculum. Wellington: Ministry of Education.
Ministry of Education. (2004). Making meaning: Making a difference. Retrieved from http://health.tki.org.nz/Key-collections/Curriculum-in-action/Making-Meaning
Ministry of Education. (2007). The New Zealand curriculum. Wellington: Ministry of Education.
Ministry of Education. (2012). Leading from the middle: Educational leadership for middle and senior leaders. Wellington: Ministry of Education.
Ministry of Education. (2013). Senior secondary guides. Retrieved from http://seniorsecondary.tki.org.nz/Health-and-physical-education/Health-education
Ministry of Education. (2014a). Alcohol and other drug education programmes guide for schools. http://health.tki.org.nz/Teaching-in-HPE/Policy-guidelines/Alcohol-and-other-drug-education-programmes
Ministry of Education. (2014b). Youth guarantee vocational pathways. Retrieved from http://youthguarantee.net.nz/vocational-pathways/
Ministry of Education. (2015). Sexuality education: A guide for principals, boards of trustees and teachers. Retrieved from http://health.tki.org.nz/Teaching-in-HPE/Policy-guidelines/Sexuality-education-a-guide-for-principals-boards-of-trustees-and-teachers
Ministry of Health. (2015). Mäori health models. Retrieved from http://www.health.govt.nz/our-work/populations/maori-health/maori-health-models
National Monitoring Study of Student Achievement (NMSSA). (2014). Health and physical education 2013. Dunedin: Educational Assessment Research Unit, University of Otago.
New Zealand Qualifications Authority. (n.d.a). Health subject resources. Retrieved from http://www.nzqa.govt.nz/qualifications-standards/qualifications/ncea/subjects/health/levels/
New Zealand Qualifications Authority. (n.d.b). National Certificate of Educational Achievement (NCEA). Retrieved from http://www.nzqa.govt.nz/qualifications-standards/qualifications/ncea/
New Zealand Qualifications Authority. (2013/2014). Secondary school statistics. Retrieved from http://www.nzqa.govt.nz/studying-in-new-zealand/secondary-school-and-ncea/find-information-about-a-school/secondary-school-statistics/
New Zealand Qualifications Authority. (2014). New Zealand Scholarship. Retrieved from http://www.nzqa.govt.nz/qualifications-standards/awards/new-zealand-scholarship/
Petrie, K., Penney, D., & Fellows, S. (2014). Health and physical education in Aotearoa New Zealand: An open market and open doors? Asia-Pacific Journal of Health, Sport and Physical Education, 5(1), 19–38.
Powell, D. & Fitzpatrick, K. (2013). “Getting fit basically means, like, non-fat”: Children’s lessons in fitness and fatness. Sport, Education and Society, 20 (4), 463–484. http://dx.doi.org/10.1080/13573322.2013.777661
Quennerstedt, M., Burrows, L., & Maivorsdotter, N. (2010). From teaching young people to be healthy to learning health. Utbildning & Demokrati, 19(2), 97–112.
Robertson, J. (2009). Mental health matters (2nd ed.). Auckland: Mental Health Foundation.
Robertson, J. & Dixon, R. (2014). Level 3 health education learning workbook. Auckland: ESA.
Robertson, J. (2005). Making sense of health promotion in context of health and physical education curriculum learning. Paper prepared for the Ministry of Education’s New Zealand Curriculum Marautanga Project. Retrieved from http://nzcurriculum.tki.org.nz/Archives/Curriculum-project-archives/References
Robertson, J. (2013). Review government-funded alcohol and other drug education programmes for young people. Retrieved from http://health.tki.org.nz/Teaching-in-HPE/Policy-guidelines/Alcohol-and-other-drug-education-programmes
Robinson, V., Hohepa, M., & Lloyd (2009). School leadership and student outcomes: Identifying what works and why—best evidence synthesis iteration (BES). Wellington, NZ: Ministry of Education.
Salter, G. (2000). Marginalising indigenous knowledge in teaching physical education: The sanitising of hauora (well-being) in the new HPE curriculum. Journal of Physical Education New Zealand, 33(1), 5–16.
Shaw H. (1994). Literature review: Health education. Retrieved from http://health.tki.org.nz/Key-collections/Curriculum-development/Health-education
Sinkinson, M., & Burrows, L. (2011). Reframing health education in New Zealand/Aotearoa schools. Asia-Pacific Journal of Health, Sport and Physical Education, 2(3/4), 53–69. http://dx.doi.org/10.1080/18377122.2011.9730359
Sinkinson, M. (2011). Back to the future: Reoccurring issues and discourses in health education in New Zealand schools. Policy Futures in Education, 9(3), 315–327. http://dx.doi.org/10.2304/pfie.2011.9.3.315
Tasker, G. (1996/97). ‘For whose benefit?’ The politics of developing a health education curriculum. Delta, 48(2)/49(1) 187–202.
Tasker, G. (1998). Caring for yourself and others: An alcohol education resource for secondary students. Christchurch: Christchurch College of Education.
Tasker, G. (2006) “It makes you think outside the square”: Examining the relationship between students’ perceptions of their learning in senior secondary health education, the proposed key competencies, the schooling strategy 2005–2010 and learning in the knowledge-rich age of the 21st century. Paper prepared for the Ministry of Education New Zealand Curriculum/Marautanga Project. Retrieved from http://nzcurriculum.tki.org.nz/Archives/Curriculum-project-archives/References
Tasker, G. (2000). Social and ethical issues in sexuality education: A resource for health education teachers of year 12 and 13 students. Christchurch: Christchurch College of Education.
Tasker, G., & Hipkins, R. (2002). Social issues: Alcohol: A resource for health education teachers of years 12 and 13 students. Christchurch: Christchurch College of Education.
Te Kete Ipurangi. (n.d). Curriculum in action (series). Retrieved from http://health.tki.org.nz/Key-collections/Curriculum-in-action
Timperley, H., McNaughton, S., Lai, M., Hohepa, Parr, J., & Dingle R. (2009). Towards an optimal model for schooling improvement: Building evaluative capability in schooling improvement project. Auckland: University of Auckland and New Zealand Council for Educational Research.
Timperley, H., Wilson, A. Barrar, H. and Fung, I. (2007). Teacher professional learning and development: Best evidence synthesis iteration (BES). Wellington: Ministry of Education.
Weir, K. J. (2009). Teaching health education in New Zealand secondary schools: Policy into practice. Unpublished PhD thesis, Massey University.
World Health Organization. (1948). World Health Organization definition of health. Retrieved from http://www.who.int/about/definition/en/print.html
World Health Organization. (1986). Ottawa Charter. Retrieved from http://www.who.int/healthpromotion/conferences/previous/ottawa/en/
World Health Organization. (2005). Bangkok Charter. Retrieved from http://www.who.int/healthpromotion/conferences/6gchp/bangkok_charter/en/
The author
Jenny Robertson currently works in a monitoring and evaluation role for English and Mäori medium schooling improvement professional learning and development contracts at The University of Auckland, Faculty of Education and Social Work. Formerly she was a secondary school teacher of science, biology and health education. Since leaving school teaching she has held health education related positions in initial teacher education and in-service professional learning and development. Jenny has also worked extensively in a range of roles that engaged her in curriculum writing, the development of teaching and learning resources, and NCEA.
Email jd.robertson@auckland.ac.nz